What Is Chronic Endometritis?
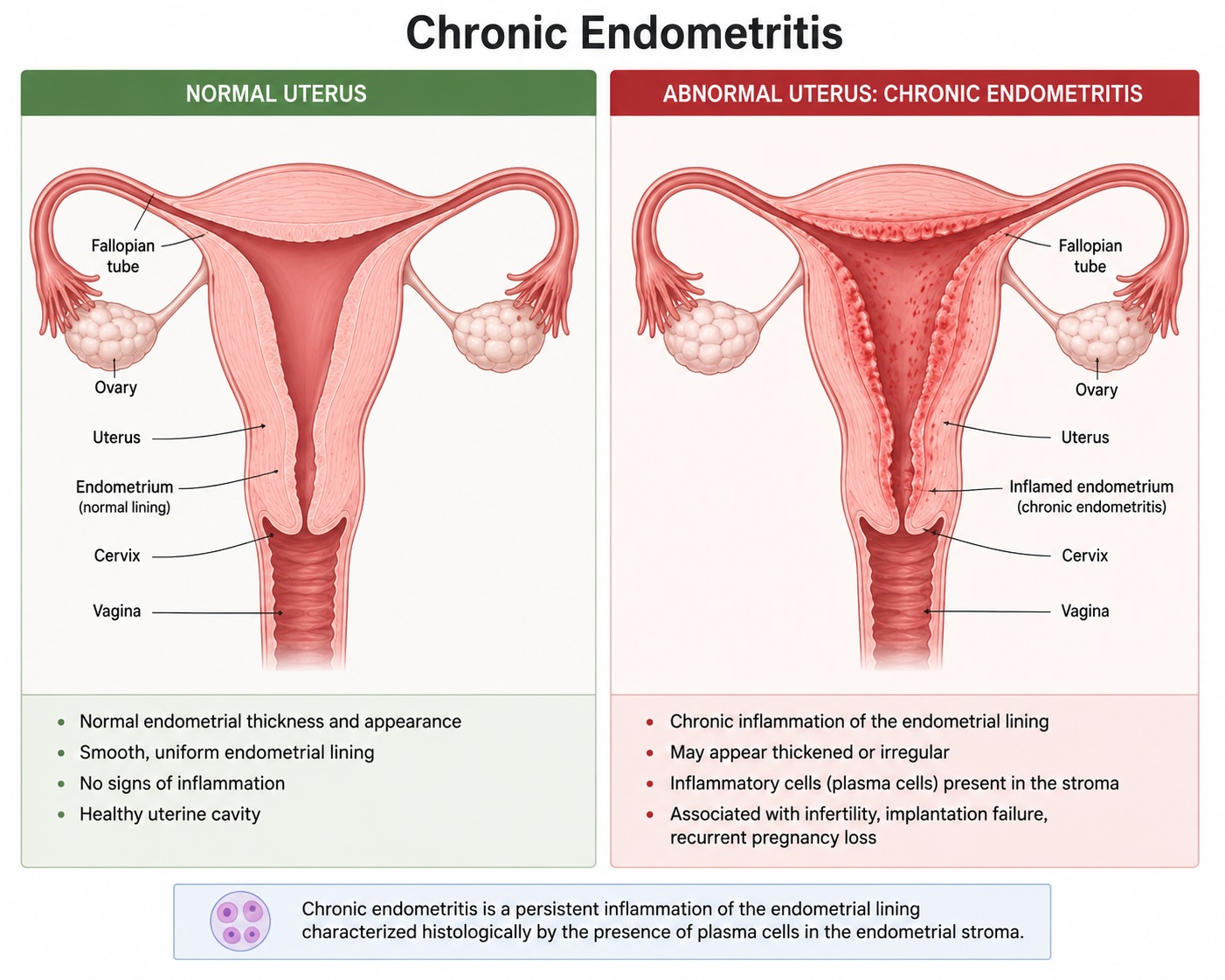
Chronic endometritis (CE) is a low-grade, persistent inflammation of the uterine lining (the endometrium). Unlike acute infections that cause obvious symptoms like fever or pain, chronic endometritis is often “silent” – most women have no symptoms at all, or only mild, nonspecific complaints such as irregular bleeding or pelvic discomfort. Because of this, it frequently goes undiagnosed.[1][2]
The inflammation is usually caused by common bacteria – such as Enterococcus, Streptococcus, E. coli, Mycoplasma, or Ureaplasma — that persist in the uterine lining and disrupt its normal function.[3]
Why Does It Matter for Fertility?
The uterine lining plays a critical role in pregnancy. For an embryo to implant successfully, the endometrium must be healthy, receptive, and have the right balance of immune cells. Chronic endometritis disrupts this environment in several ways:
– It alters the immune cells in the uterine lining, creating a hostile environment for an embryo trying to implant.[1][2]
– It impairs the lining’s ability to prepare for pregnancy (a process called decidualization).[2]
– It disrupts the natural balance of bacteria in the uterus, which can further reduce receptivity.[1]
Research shows that CE is found in up to 30–40% of women with unexplained infertility, recurrent implantation failure (RIF) after IVF, or recurrent pregnancy loss. A large meta-analysis found that infertile women are about three times more likely to have CE compared to fertile women.[3][4][5][6]
How Is Chronic Endometritis Diagnosed?
Because CE is usually invisible on ultrasound and causes few or no symptoms, specialized testing is needed. The two main diagnostic approaches are:
- Office Hysteroscopy: A thin, lighted camera is gently passed through the cervix to directly visualize the inside of the uterus. This is typically done in the office without general anesthesia. During hysteroscopy, your doctor looks for telltale signs of CE, including:
– Redness or increased blood flow in the lining (hyperemia)
– Swelling of the tissue (stromal edema)
– Tiny polyp-like growths called micropolyps
– A “strawberry-like” appearance of the lining
Recent large studies have shown that hysteroscopy is highly accurate for detecting CE, with a sensitivity of about 82–84% and specificity of about 81–89%. This means that if the uterine lining looks normal during hysteroscopy, CE is very unlikely.[7][8] However, if suspicious findings are seen, a tissue sample (biopsy) is recommended to confirm the diagnosis.[7][9]
- Endometrial Biopsy with Special Staining: During or after hysteroscopy, a small sample of the uterine lining is taken. The tissue is examined under a microscope using a special stain called CD138, which highlights plasma cells — a type of immune cell that is the hallmark of chronic endometritis. Finding a certain number of these cells (typically 5 or more per 10 microscopic fields) confirms the diagnosis.[5][9]
The combination of office hysteroscopy and biopsy is considered the most thorough approach. Hysteroscopy allows your doctor to see the uterus directly and identify other potential problems (such as polyps, fibroids, or scar tissue), while the biopsy provides definitive confirmation of inflammation.[3][7]
The Dual Benefit of Office Hysteroscopy: Diagnosis and Treatment
Office hysteroscopy offers more than just a diagnosis. The procedure itself may have therapeutic benefits:
– Identifying and treating other problems: During hysteroscopy, your doctor can remove polyps, small fibroids, or scar tissue — all of which are associated with CE and can independently reduce fertility. Studies have shown that removing endometrial polyps alone can cure CE in approximately 85–90% of cases, even without antibiotics.[10][11]
– Guiding targeted treatment: By combining visual inspection with tissue sampling, your doctor can tailor antibiotic therapy specifically to your situation rather than treating blindly.[3]
How Is Chronic Endometritis Treated?
Once CE is confirmed, treatment typically involves a course of oral antibiotics. The most commonly used options include:
– Doxycycline (100 mg twice daily for 14 days) — the most widely used first-line treatment[5][12]
– Ciprofloxacin and Flagyl (for 14 days) — an alternative regimen
Studies show that approximately 70–90% of women are cured after one course of antibiotics. For the small percentage of women who do not respond to the first course, a second round of antibiotics — sometimes with a different combination — is effective in the majority of remaining cases, with cumulative cure rates reaching approximately 88%.[5][12]
After treatment, many doctors recommend a follow-up biopsy to confirm that the inflammation has resolved before proceeding with fertility treatment.[4][5]
Does Treating CE Actually Improve Pregnancy Outcomes?
This is the most important question, and the evidence is encouraging:
– Women whose CE was successfully treated had live birth rates of about 34%, compared to only about 6% in women whose CE was left untreated.[12]
– After successful treatment, pregnancy rates in women who previously had CE were comparable to those of women who never had CE in the first place.[5][12]
– In women with recurrent implantation failure, one study found that those whose CE was cured had a clinical pregnancy rate of 65% and a live birth rate of 61% in their next IVF cycle, compared to 33% and 13% in women with persistent CE.[4]
– A systematic review and meta-analysis found that women with cured CE had significantly higher ongoing pregnancy and live birth rates compared to those with persistent CE (OR 6.82, p 0.00001).[13]
It is important to note that while these results are encouraging, some experts have highlighted that diagnostic criteria remain heterogeneous across studies, and large prospective trials are still needed to fully define the impact of CE treatment in the general infertile population.[14]
What to Expect During an Office Hysteroscopy
– The procedure is typically performed in your doctor’s office, without general anesthesia.
– It usually takes 10–15 minutes.
– You may experience mild cramping similar to menstrual cramps during and briefly after the procedure.
– Over-the-counter pain medication (such as ibuprofen) taken before the procedure can help with discomfort.
– Most women return to normal activities the same day.
– Complications are rare (less than 1–2%) and may include mild bleeding or, very rarely, infection.
Key Takeaways
– Chronic endometritis is a common but often hidden cause of infertility and failed IVF cycles.[3][6]
– Office hysteroscopy combined with endometrial biopsy is a safe, effective, and minimally invasive way to diagnose CE — and can also treat other uterine problems at the same time.[7][8][10]
– Antibiotic treatment is highly effective at curing CE, and successful treatment has been shown to significantly improve pregnancy and live birth rates.[4][12][13]
– If you have experienced unexplained infertility, repeated IVF failures, or recurrent pregnancy loss, ask your doctor whether evaluation for chronic endometritis may be appropriate for you.
References
- Inflammatory Mechanisms and Therapeutic Advances in Chronic Endometritis. Yan X, Jiao J, Wang X. Frontiers in Immunology. 2025;16:1616217. doi:10.3389/fimmu.2025.1616217.
- The Pathogenesis, Diagnosis, and Treatment of Chronic Endometritis: A Comprehensive Review. Yan X, Jiao J, Wang X. Frontiers in Endocrinology. 2025;16:1603570. doi:10.3389/fendo.2025.1603570.
- The Diagnosis of Chronic Endometritis in Infertile Asymptomatic Women: A Comparative Study of Histology, Microbial Cultures, Hysteroscopy, and Molecular Microbiology. Moreno I, Cicinelli E, Garcia-Grau I, et al. American Journal of Obstetrics and Gynecology. 2018;218(6):602.e1-602.e16. doi:10.1016/j.ajog.2018.02.012.
- Prevalence of Chronic Endometritis in Repeated Unexplained Implantation Failure and the IVF Success Rate After Antibiotic Therapy. Cicinelli E, Matteo M, Tinelli R, et al. Human Reproduction (Oxford, England). 2015;30(2):323-30. doi:10.1093/humrep/deu292.
- Chronic Endometritis Identified by Plasma Cells Can Often Be Diagnosed in Patients With Recurrent Implantation Failure. Amrani M, Renné C, Blaschke V, et al. European Journal of Obstetrics, Gynecology, and Reproductive Biology. 2025;312:114092. doi:10.1016/j.ejogrb.2025.114092.
- Chronic Endometritis and Recurrent Reproductive Failure: A Systematic Review and Meta-Analysis. Ticconi C, Inversetti A, Marraffa S, et al. Frontiers in Immunology. 2024;15:1427454. doi:10.3389/fimmu.2024.1427454.
- Hysteroscopic Criteria for the Diagnosis of Chronic Endometritis: A Systematic Review and Diagnostic Test Accuracy Meta-Analysis. Riemma G, Parry JP, De Franciscis P, et al. American Journal of Obstetrics and Gynecology. 2025;233(1):12-24.e4. doi:10.1016/j.ajog.2025.03.005.
- Diagnostic Accuracy of Hysteroscopy for Chronic Endometritis in Reproductive-Age and Infertile Women: A Systematic Review and Latent Class Meta-Analysis. Pérez Milán F, Caballero Campo M, Domínguez Arroyo JA, et al. Journal of Minimally Invasive Gynecology. 2026;:S1553-4650(26)00128-7. doi:10.1016/j.jmig.2026.02.021.
- Correlation Between Hysteroscopy Findings and Chronic Endometritis. Song D, Li TC, Zhang Y, et al. Fertility and Sterility. 2019;111(4):772-779. doi:10.1016/j.fertnstert.2018.12.007.
- Prevalence of and Risk Factors for Chronic Endometritis in Patients With Intrauterine Disorders After Hysteroscopic Surgery. Kuroda K, Yamanaka A, Takamizawa S, et al. Fertility and Sterility. 2022;118(3):568-575. doi:10.1016/j.fertnstert.2022.05.029.
- Comparison of Resectoscope and Tissue Removal Device in Managing Chronic Endometritis Associated With Endometrial Polyps. Kuroda K, Kuribayashi Y, Moriyama A, et al. Journal of Reproductive Immunology. 2026;175:104878. doi:10.1016/j.jri.2026.104878.
- Chronic Endometritis: Screening, Treatment, and Pregnancy Outcomes in an Academic Fertility Center. HogenEsch E, Hojjati R, Komorowski A, et al. Journal of Assisted Reproduction and Genetics. 2023;40(10):2463-2471. doi:10.1007/s10815-023-02902-z.
- Impact of Antibiotic Treatment for Chronic Endometritis on Pregnancy Outcomes in Women With Reproductive Failures (RIF and RPL): A Systematic Review and Meta-Analysis. Liu J, Liu ZA, Liu Y, Cheng L, Yan L. Frontiers in Medicine. 2022;9:980511. doi:10.3389/fmed.2022.980511.
- Chronic Endometritis, Chronic Questions: A Narrative Review of Current Practices. Reig A. Current Opinion in Obstetrics & Gynecology. 2025;:00001703-990000000-00198. doi:10.1097/GCO.0000000000001053.



