procedures offered
Pudendal neuralgia is a condition that causes chronic pain in the pelvic area. It happens when the pudendal nerve — a major nerve that runs through the pelvis and provides sensation to the genitals, perineum (the area between the genitals and anus), and rectum — becomes irritated, inflamed, or compressed.
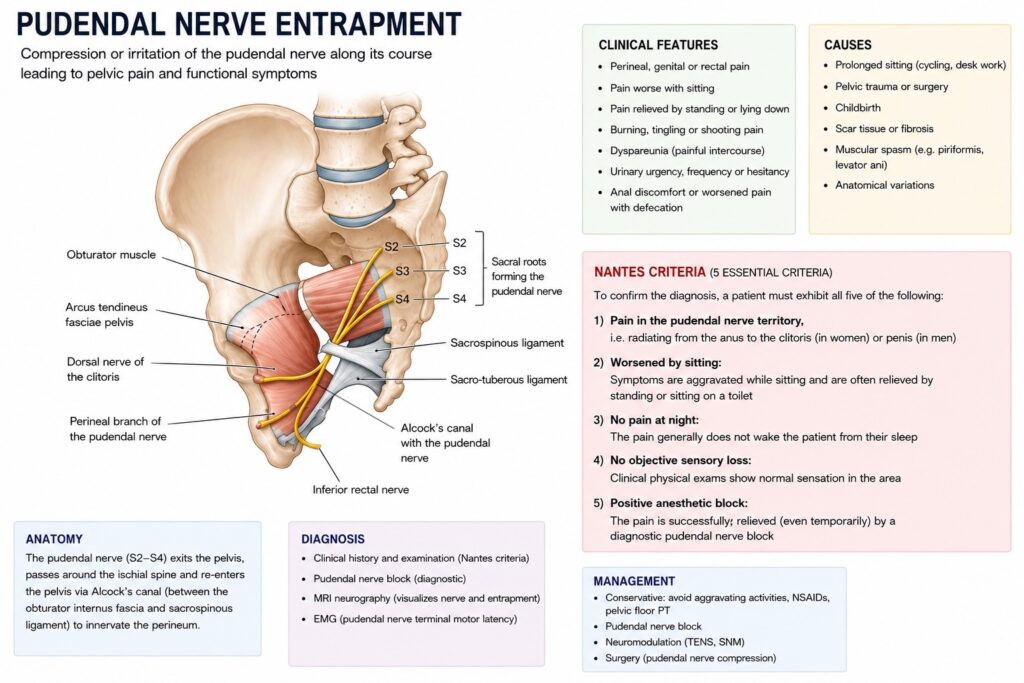
When the pain is caused by the nerve being physically squeezed or trapped along its path, this is called pudendal nerve entrapment. The nerve most commonly becomes trapped between two ligaments deep in the pelvis (the sacrospinous and sacrotuberous ligaments), or within a small tunnel called Alcock’s canal.
The exact cause is not always clear, but common contributing factors include:
The hallmark symptom is pain in the area supplied by the pudendal nerve. Common symptoms include:
Symptoms can affect one or both sides and may significantly impact quality of life.
Pudendal neuralgia is primarily diagnosed based on your symptoms and a physical examination. Doctors use a set of criteria called the Nantes criteria to help confirm the diagnosis. All five of the following should be present:
The pudendal nerve block is an important diagnostic step. A small amount of local anesthetic is injected near the nerve using image guidance (such as CT or ultrasound). If the injection temporarily relieves your pain, it strongly supports the diagnosis.
Additional tests may sometimes be used, including:
Treatment follows a stepwise approach, starting with the least invasive options and progressing if needed.
Cognitive behavioral therapy (CBT) and other psychological approaches can help manage chronic pain and its impact on daily life
When conservative treatments have not provided adequate relief, surgery to free the trapped nerve may be recommended. The goal of surgery is to release the nerve from the structures compressing it, allowing it to function normally again. There are several surgical approaches:
This is a minimally invasive approach performed through small incisions in the abdomen. Using a camera and specialized instruments, the surgeon works from inside the pelvis to identify the pudendal nerve and carefully release it by cutting the ligaments or tissues that are compressing it.
Advantages of the laparoscopic approach:
This approach accesses the nerve through an incision in the buttock. The surgeon works through the gluteal muscles to reach the pudendal nerve and release it from its entrapment.
Advantages of the transgluteal approach:
Both laparoscopic and transgluteal approaches aim to achieve the same goal: freeing the pudendal nerve from compression. A recent analysis of published studies found that the laparoscopic approach had a higher rate of significant pain relief (approximately 91%) compared to the transgluteal approach (approximately 50%), though direct comparison is difficult because the studies used different patient selection criteria and follow-up periods.
The transgluteal approach has the advantage of longer-term evidence and is the only approach supported by a randomized controlled trial. It also provides access to the cluneal nerves if they are involved. The laparoscopic approach offers the benefits of minimally invasive surgery, including smaller incisions, excellent visualization, and a shorter recovery. However, it requires advanced laparoscopic surgical skills.
Your surgeon will recommend the approach that is best suited to your specific situation, taking into account the location of nerve compression, your anatomy, and their expertise.
If you have questions about your diagnosis or treatment options, please discuss them with your healthcare team.