How Do Endometriosis and Adenomyosis Affect Fertility?
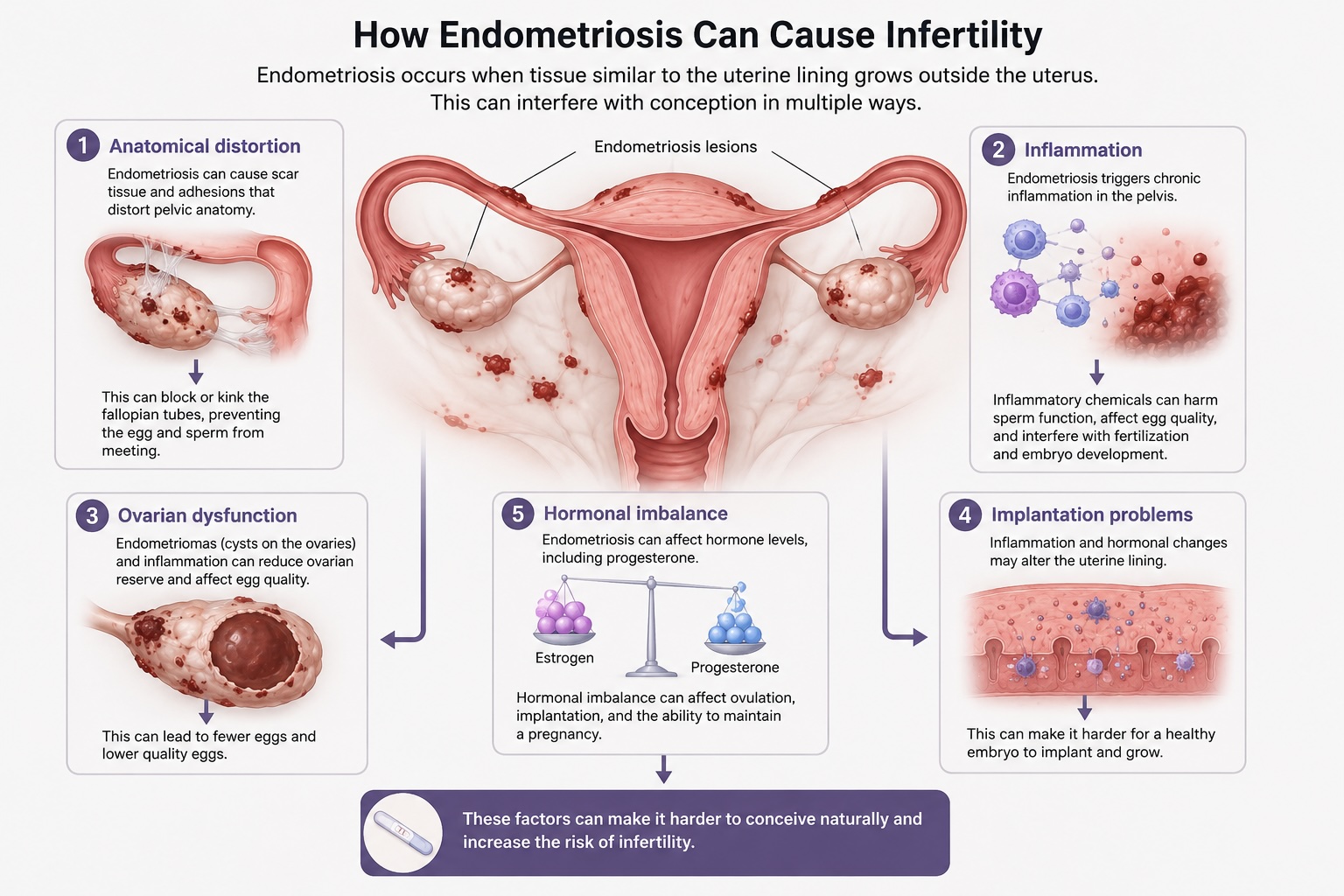
Endometriosis is a condition in which tissue similar to the lining of the uterus grows outside the uterus — often on the ovaries, fallopian tubes, and surrounding pelvic structures. It is one of the most common causes of infertility, affecting approximately 30–50% of women with the condition.[1] Endometriosis can reduce fertility in several ways: it can distort the normal anatomy of the pelvis through scar tissue and adhesions, interfere with the function of the fallopian tubes and ovaries, create inflammation that harms egg quality and embryo development, and alter the uterine lining in ways that make it harder for an embryo to implant.
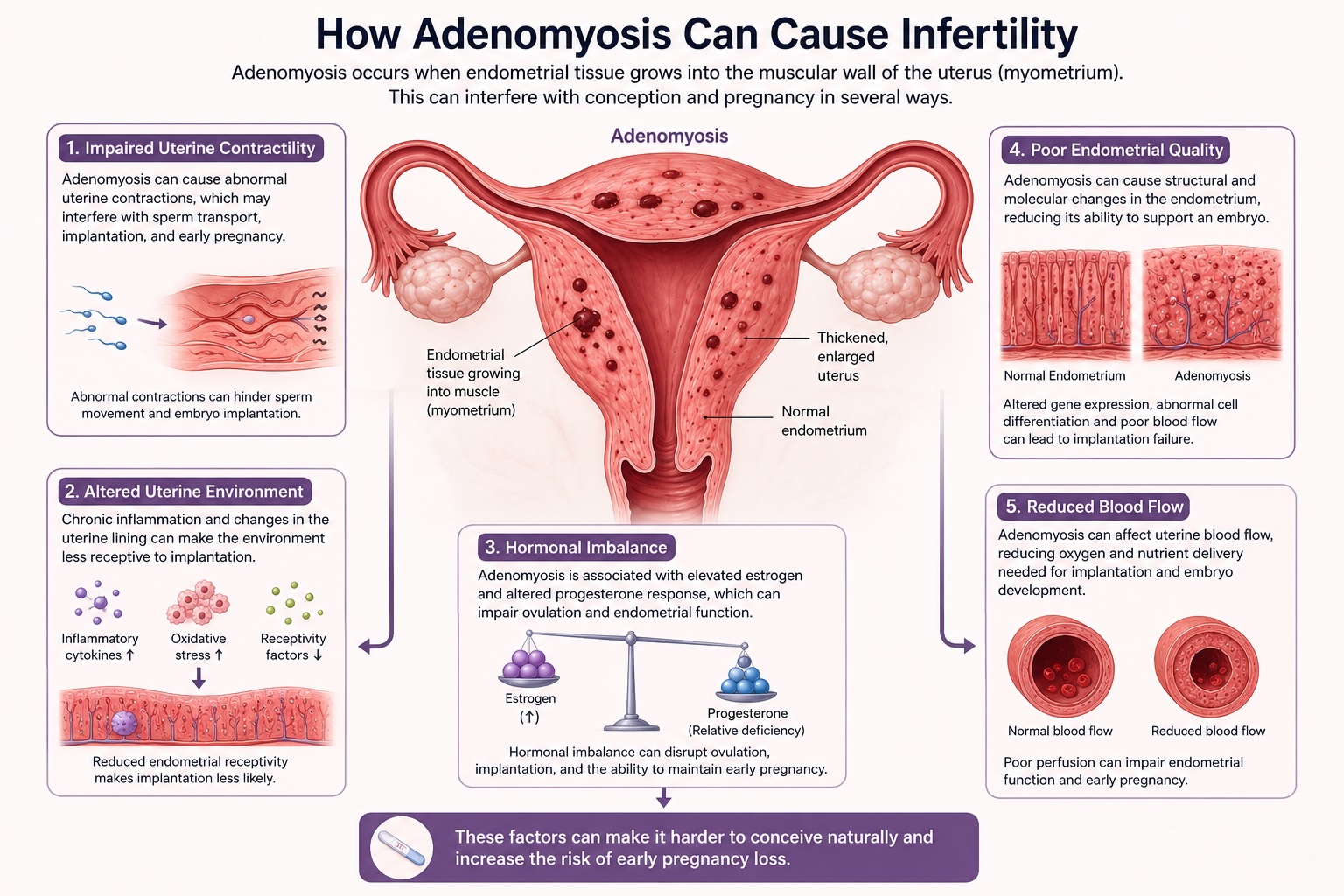
Adenomyosis is a related condition in which tissue similar to the uterine lining grows into the muscular wall of the uterus itself. Adenomyosis is increasingly recognized as a contributor to infertility and is found in a significant number of women undergoing fertility treatment. Research shows that women with adenomyosis have lower rates of embryo implantation, lower clinical pregnancy rates, and a higher risk of miscarriage compared to women without the condition. In studies of women undergoing IVF, adenomyosis has been associated with approximately a 28% reduction in the likelihood of clinical pregnancy and a doubled miscarriage rate, as well as a roughly 30–40% reduction in live birth rates.[2][3][4] Adenomyosis and endometriosis frequently coexist, and when both are present, the impact on fertility may be even greater.
Surgery for Endometriosis: When Does It Help Fertility?
For women with endometriosis-related infertility, surgery to remove endometriosis lesions, scar tissue, and cysts (endometriomas) can improve the chances of natural conception — particularly in women with moderate-to-severe disease. The American Society for Reproductive Medicine (ASRM) recommends either conservative surgery or IVF for women with stage III/IV endometriosis who wish to conceive.[5]
However, surgery is not always the best first step. Research has shown that removing ovarian endometriomas (cysts on the ovaries) does not clearly improve IVF success rates and can reduce ovarian reserve — meaning the ovaries may respond less well to fertility medications afterward. A recent large review of 22 studies and over 3,500 women found that performing surgery before IVF did not significantly improve live birth rates for women with ovarian endometriomas or deep endometriosis, and surgery was associated with lower egg counts and reduced ovarian reserve markers.[6] For this reason, the decision to operate must be carefully weighed against the potential impact on future fertility treatment.
Surgery may still be recommended in certain situations — for example, if an endometrioma is large (greater than 4 cm), if there is a need to confirm the diagnosis, if pain symptoms need to be addressed, or if surgery is needed to allow safe access to the ovaries during an egg retrieval procedure.[5] If a first surgery does not lead to pregnancy, repeat surgery is generally less effective than proceeding to IVF.[5]
The Role of IVF in Endometriosis-Related Infertility
In vitro fertilization (IVF) is considered the most effective treatment for endometriosis-related infertility, particularly for women with moderate-to-severe disease, older women, or those who have not conceived after surgery.[1] Data from large national databases show that IVF outcomes for women with endometriosis are broadly comparable to outcomes for other causes of infertility.
One important strategy that may improve IVF success in women with endometriosis is a period of hormonal suppression before starting an IVF cycle. Treatment with a GnRH agonist (a medication that temporarily suppresses estrogen) for 3–6 months, or continuous birth control pills for 6–8 weeks before IVF, has been shown to significantly increase pregnancy rates.[1][7] This approach is thought to work by reducing the inflammation and hormonal disruption caused by endometriosis, creating a more favorable environment for embryo implantation.
Adenomyosis and Fertility Treatment
For women with adenomyosis, the path to pregnancy can be more complex. Because adenomyosis affects the uterine muscle and lining, it can impair embryo implantation and increase the risk of miscarriage — even with IVF. Studies have consistently shown that women with adenomyosis have lower live birth rates and higher miscarriage rates during IVF treatment compared to women without the condition.[2][3]
Treatment strategies for adenomyosis-related infertility are still evolving. Some evidence suggests that using a long-protocol GnRH agonist regimen before a frozen embryo transfer may improve outcomes by suppressing the adenomyosis and creating a more receptive uterine environment.[4][8] In selected cases — particularly when adenomyosis is focal (localized to one area) — surgical removal of the adenomyotic tissue (adenomyomectomy) has been reported to improve pregnancy rates, though this approach carries risks including uterine rupture in a future pregnancy and is not yet supported by large randomized trials.[9] For women with diffuse adenomyosis, the evidence for surgical benefit is less clear.
If you have been diagnosed with adenomyosis, it is important to discuss with your fertility specialist how this may affect your treatment plan and what steps can be taken to optimize your chances.
When IVF Has Not Worked: Can Surgery Help After Repeated Failed Embryo Transfers?
For women with endometriosis or adenomyosis who have undergone two or more IVF cycles without a successful pregnancy, surgery may be worth considering as a way to improve the chances of success with future IVF attempts. While IVF is generally the preferred treatment after a failed surgical attempt, the reverse scenario — turning to surgery after repeated IVF failures — is an area of growing interest and research.
Endometriosis surgery after failed IVF. Several studies have examined whether surgical treatment of endometriosis can “reset” the pelvic environment and improve IVF outcomes in women who have already failed multiple cycles. In one study of 78 women with severe endometriosis (stage III/IV) who had all experienced repeated IVF failures, laparoscopic surgery led to a delivery rate of 42.3% — with the vast majority of those pregnancies achieved through IVF after the surgery. Women who were younger (average age 32.5 vs. 35.5 years) and who had adequate ovarian reserve were most likely to benefit. Salpingectomy (removal of damaged fallopian tubes) performed during surgery was also associated with a trend toward improved delivery rates.[10]
A larger study from a French multicenter database looked specifically at women with deep infiltrating endometriosis who had experienced at least two prior IVF/ICSI failures. After complete surgical excision of the endometriosis, the postoperative pregnancy rate was 43.8%, with most pregnancies occurring within the first year after surgery. About one in five of those pregnancies occurred spontaneously, without any further fertility treatment. Younger age (under 35) and avoiding additional ovarian surgery were associated with the best outcomes.[11]
A meta-analysis focused on deep infiltrating endometriosis found that women who had surgery before IVF had significantly higher pregnancy rates per patient and live birth rates per patient compared to those who went directly to IVF — with the live birth rate more than doubled. However, it is important to note that these studies are observational, not randomized controlled trials, and the results should be interpreted with some caution. A more recent and broader meta-analysis found that surgery before IVF did not significantly improve live birth rates overall, underscoring the importance of careful patient selection.[6]
Adenomyosis surgery after failed IVF. For women with adenomyosis and repeated implantation failures, the evidence for surgery is more limited but emerging. One approach involves laparoscopic adenomyomectomy — surgical removal of the adenomyotic tissue — which has shown pregnancy rates above 50% and live birth rates of up to 70% in women with focal (localized) adenomyosis.[9] Research suggests that adenomyomectomy may be most beneficial for women under 39 years of age with focal disease. For women aged 40 and older, or those with diffuse adenomyosis, the benefit of surgery is less certain, and the risks — including uterine rupture in a future pregnancy (reported in up to 6% of cases) — must be carefully weighed.[9]
Treatment strategies for adenomyosis-related infertility are still evolving, and some emerging approaches — such as hysteroscopic treatment of adenomyotic cystic lesions — have shown promise in small case series of women with multiple IVF failures, though more research is needed.
Who might benefit from surgery after failed IVF? Not every woman with failed embryo transfers will benefit from surgery. The best candidates tend to be:
– Women with known or suspected severe endometriosis (stage III/IV) or deep infiltrating endometriosis, especially if they also have pain symptoms
– Women with focal adenomyosis or adenomyotic cysts that persist after medical treatment
– Women who are younger (generally under 35–39 years of age)
– Women who have adequate ovarian reserve
– Women with hydrosalpinges (fluid-filled, blocked fallopian tubes), where removal of the affected tube before IVF has been clearly shown to improve pregnancy and live birth rates
It is essential that surgery in this setting be performed by a highly experienced surgical team specializing in advanced endometriosis and/or adenomyosis. The goal is to reduce inflammation, remove disease that may be interfering with implantation, and optimize the pelvic environment — while preserving as much ovarian function as possible. Your fertility specialist and surgeon can help determine whether surgery is a reasonable next step in your individual situation. Dr. Einarsson works closely with the fertility experts at Sunna Fertility https://sunnafrjosemi.is/sunna-fertility/ who provide an outstanding service to patients with infertility due to endometriosis, adenomyosis and other conditions.
What Is the Endometriosis Fertility Index (EFI)?
The Endometriosis Fertility Index, or EFI, is a scoring tool that your surgeon can calculate after surgery for endometriosis. It was specifically designed to estimate the likelihood of becoming pregnant without the need for IVF or other assisted reproductive technologies. The EFI is scored on a scale of 0 to 10 and takes into account several important factors: your age, how long you have been trying to conceive, whether you have been pregnant before, the severity of the endometriosis found during surgery, and — most importantly — how well the fallopian tubes and ovaries are functioning at the end of the procedure.[12] The EFI has been validated in multiple studies across different countries and populations, confirming that it reliably predicts the chance of natural pregnancy after surgery.
What Do the EFI Scores Mean?
Research involving thousands of women has shown a clear relationship between EFI scores and pregnancy rates. A large review combining data from 17 studies and over 4,500 women found that the chance of becoming pregnant without IVF within three years of surgery ranged from about 10% for women with the lowest scores (EFI 0–2) to approximately 69% for women with the highest scores (EFI 9–10). Women with scores in the middle range (EFI 5–6) had roughly a 44% chance, while those with scores of 7–8 had about a 55% chance.[13] Another study focusing specifically on moderate-to-severe endometriosis found that women with an EFI of 9–10 had a cumulative live birth rate without IVF as high as 91% over five years, while those with an EFI of 0–2 did not achieve a live birth without assisted reproduction.[14]
How the EFI Guides Your Next Steps: Surgery, Natural Conception, or IVF?
The EFI is a valuable tool for deciding what to do after surgery. If your EFI score is favorable (generally 7 or higher), the evidence suggests that trying to conceive naturally for up to 12–24 months after surgery is a reasonable approach, since most pregnancies in this group occur within that window. If your EFI score is low (4 or below), studies suggest that the chance of natural pregnancy is significantly lower and that earlier referral to IVF or other fertility treatments may lead to better outcomes.[15]
Your doctor will also consider other factors when recommending a treatment plan, including your age, your partner’s fertility, whether you also have adenomyosis, your ovarian reserve, and your personal goals. For women over 35, or those with additional fertility factors, a more proactive approach — such as proceeding to IVF sooner — may be recommended, since both endometriosis and age can independently reduce fertility.
It is important to remember that the EFI is one piece of the puzzle. The best treatment plan is one that is individualized to your specific situation. If you have questions about your EFI score, your endometriosis or adenomyosis diagnosis, or what treatment path is right for you, your reproductive specialist can walk you through your individual results and options.
References
- Vesali S, Razavi M, Rezaeinejad M, et al. Endometriosis Fertility Index for Predicting Non-Assisted Reproductive Technology Pregnancy After Endometriosis Surgery: A Systematic Review and Meta-Analysis. BJOG. 2020;127(7):800-809.
- Tomassetti C, Geysenbergh B, Meuleman C, et al. External Validation of the Endometriosis Fertility Index (EFI) Staging System for Predicting Non-ART Pregnancy After Endometriosis Surgery. Human Reproduction. 2013;28(5):1280-1288.
- Maheux-Lacroix S, Nesbitt-Hawes E, Deans R, et al. Endometriosis Fertility Index Predicts Live Births Following Surgical Resection of Moderate and Severe Endometriosis. Human Reproduction. 2017;32(11):2243-2249.
- Bailleul A, Niro J, Du Cheyron J, Panel P, Fauconnier A. Infertility Management According to the Endometriosis Fertility Index in Patients Operated for Endometriosis: What Is the Optimal Time Frame? PLoS One. 2021;16(5):e0251372.
- Taylor HS, Kotlyar AM, Flores VA. Endometriosis Is a Chronic Systemic Disease: Clinical Challenges and Novel Innovations. Lancet. 2021;397(10276):839-852.
- Riemma G, García-Velasco JA, Abrão MS, et al. IVF/ICSI or Surgery as First Approach for the Treatment of Infertility Associated With Ovarian and Deep Infiltrating Endometriosis? A Systematic Review and Meta-Analysis. Reproductive Biomedicine Online. 2025;52(2):105178.
- Practice Committee of the American Society for Reproductive Medicine. Endometriosis and Infertility: A Committee Opinion. Fertility and Sterility. 2012;98(3):591-598.
- Georgiou EX, Melo P, Baker PE, et al. Long-Term GnRH Agonist Therapy Before In Vitro Fertilisation (IVF) for Improving Fertility Outcomes in Women With Endometriosis. Cochrane Database of Systematic Reviews. 2019;(11):CD013240.
- Vercellini P, Consonni D, Dridi D, et al. Uterine Adenomyosis and In Vitro Fertilization Outcome: A Systematic Review and Meta-Analysis. Human Reproduction. 2014;29(5):964-977.
- Bourdon M, Mimouni A, Maignien C, et al. Reduced Live Birth Rates Following ART in Adenomyosis Patients: A Matched Control Study. Human Reproduction. 2025;40(5):855-864.
- Younes G, Tulandi T. Effects of Adenomyosis on In Vitro Fertilization Treatment Outcomes: A Meta-Analysis. Fertility and Sterility. 2017;108(3):483-490.
- Ioannidou A, Louis K, Sioutis D, et al. Conservative Surgical Management of Adenomyosis: Implications for Infertility and Pregnancy Outcomes — A Perspective Review. Journal of Clinical Medicine. 2025;14(19):6956.
- French HM, Zhang W, Movilla PR, Isaacson KB, Morris SN. Adenomyosis and Fertility: Does Adenomyosis Impact Fertility and Does Treatment Improve Outcomes. Current Opinion in Obstetrics Gynecology. 2022;34(4):227-236.
- Soriano D, Adler I, Bouaziz J, et al. Fertility Outcome of Laparoscopic Treatment in Patients With Severe Endometriosis and Repeated In Vitro Fertilization Failures. Fertility and Sterility. 2016;106(5):1264-1269.
- Breteau P, Chanavaz-Lacheray I, Rubod C, et al. Pregnancy Rates After Surgical Treatment of Deep Infiltrating Endometriosis in Infertile Patients With at Least 2 Previous In Vitro Fertilization or Intracytoplasmic Sperm Injection Failures. Journal of Minimally Invasive Gynecology. 2020;27(5):1148-1157.
- Casals G, Carrera M, Domínguez JA, Abrão MS, Carmona F. Impact of Surgery for Deep Infiltrative Endometriosis Before In Vitro Fertilization: A Systematic Review and Meta-Analysis. Journal of Minimally Invasive Gynecology. 2021;28(7):1303-1312.
- Li JJ, Chung JPW, Wang S, Li TC, Duan H. The Investigation and Management of Adenomyosis in Women Who Wish to Improve or Preserve Fertility. BioMed Research International. 2018;2018:6832685.
- Di Spiezio Sardo A, Iorio GG, Guerra S, et al. The Role of Hysteroscopy in Patients With Adenomyosis and Infertility: Bringing Out the Submerged. Fertility and Sterility. 2025;123(6):1140-1142.
- Practice Committee of the American Society for Reproductive Medicine. Role of Tubal Surgery in the Era of Assisted Reproductive Technology: A Committee Opinion. Fertility and Sterility. 2021;115(5):1143-1150.
- Melo P, Georgiou EX, Johnson N, et al. Surgical Treatment for Tubal Disease in Women Due to Undergo In Vitro Fertilisation. Cochrane Database of Systematic Reviews. 2020;10:CD002125.
References
- Endometriosis Is a Chronic Systemic Disease: Clinical Challenges and Novel Innovations. Taylor HS, Kotlyar AM, Flores VA. Lancet (London, England). 2021;397(10276):839-852. doi:10.1016/S0140-6736(21)00389-5.
- Uterine Adenomyosis and in Vitro Fertilization Outcome: A Systematic Review and Meta-Analysis. Vercellini P, Consonni D, Dridi D, et al. Human Reproduction (Oxford, England). 2014;29(5):964-77. doi:10.1093/humrep/deu041.
- Reduced Live Birth Rates Following ART in Adenomyosis Patients: A Matched Control Study. Bourdon M, Mimouni A, Maignien C, et al. Human Reproduction (Oxford, England). 2025;40(5):855-864. doi:10.1093/humrep/deaf052.
- Effects of Adenomyosis on In vitro Fertilization Treatment Outcomes: A Meta-Analysis. Younes G, Tulandi T. Fertility and Sterility. 2017;108(3):483-490.e3. doi:10.1016/j.fertnstert.2017.06.025.
- Endometriosis and Infertility: A Committee Opinion. Fertility and Sterility. 2012;98(3):591-8. doi:10.1016/j.fertnstert.2012.05.031.
- IVF/ICSI or Surgery as First Approach for the Treatment of Infertility Associated With Ovarian and Deep Infiltrating Endometriosis? A Systematic Review and Meta-Analysis. Riemma G, García-Velasco JA, Abrão MS, et al. Reproductive Biomedicine Online. 2025;52(2):105178. doi:10.1016/j.rbmo.2025.105178.
- Long-Term GnRH Agonist Therapy Before in Vitro Fertilisation (IVF) for Improving Fertility Outcomes in Women With Endometriosis. Georgiou EX, Melo P, Baker PE, et al. The Cochrane Database of Systematic Reviews. 2019;2019(11). doi:10.1002/14651858.CD013240.pub2.
- Adenomyosis and Fertility: Does Adenomyosis Impact Fertility and Does Treatment Improve Outcomes. French HM, Zhang W, Movilla PR, Isaacson KB, Morris SN. Current Opinion in Obstetrics & Gynecology. 2022;34(4):227-236. doi:10.1097/GCO.0000000000000789.
- Conservative Surgical Management of Adenomyosis: Implications for Infertility and Pregnancy Outcomes-a Perspective Review. Ioannidou A, Louis K, Sioutis D, et al. Journal of Clinical Medicine. 2025;14(19):6956. doi:10.3390/jcm14196956.
- Fertility Outcome of Laparoscopic Treatment in Patients With Severe Endometriosis and Repeated In vitro Fertilization Failures. Soriano D, Adler I, Bouaziz J, et al. Fertility and Sterility. 2016;106(5):1264-1269. doi:10.1016/j.fertnstert.2016.06.003.
- Pregnancy Rates After Surgical Treatment of Deep Infiltrating Endometriosis in Infertile Patients With at Least 2 Previous in Vitro Fertilization or Intracytoplasmic Sperm Injection Failures. Breteau P, Chanavaz-Lacheray I, Rubod C, et al. Journal of Minimally Invasive Gynecology. 2020 Jul – Aug;27(5):1148-1157. doi:10.1016/j.jmig.2019.08.032.
- External Validation of the Endometriosis Fertility Index (EFI) Staging System for Predicting Non-Art Pregnancy After Endometriosis Surgery. Tomassetti C, Geysenbergh B, Meuleman C, et al. Human Reproduction (Oxford, England). 2013;28(5):1280-8. doi:10.1093/humrep/det017.
- Endometriosis Fertility Index for Predicting Non-Assisted Reproductive Technology Pregnancy After Endometriosis Surgery: A Systematic Review and Meta-Analysis. Vesali S, Razavi M, Rezaeinejad M, et al. BJOG : An International Journal of Obstetrics and Gynaecology. 2020;127(7):800-809. doi:10.1111/1471-0528.16107.
- Endometriosis Fertility Index Predicts Live Births Following Surgical Resection of Moderate and Severe Endometriosis. Maheux-Lacroix S, Nesbitt-Hawes E, Deans R, et al. Human Reproduction (Oxford, England). 2017;32(11):2243-2249. doi:10.1093/humrep/dex291.
- Infertility Management According to the Endometriosis Fertility Index in Patients Operated for Endometriosis: What Is the Optimal Time Frame?. Bailleul A, Niro J, Du Cheyron J, Panel P, Fauconnier A. PloS One. 2021;16(5):e0251372. doi:10.1371/journal.pone.0251372.



